Diabetes Mellitus (Type 2)
Diabetes Mellitus is part of a group of metabolic diseases. It is a disease of chronic hyperglycaemia due to insulin deficiency, resistance, or both. The result is the body’s ability to use glucose for energy is impaired. While the causes and effects of type 1 and type 2 diabetes are different, the long-term effects are the same.
Diabetes Mellitus is part of a group of metabolic diseases. It is a disease of chronic hyperglycaemia due to insulin deficiency, resistance, or both. The result is the body’s ability to use glucose for energy is impaired. While the causes and effects of type 1 and type 2 diabetes are different, the long-term effects are the same. Type 1 is believed to be an autoimmune response resulting in a complete lack of insulin, whereas with type 2, the body is still producing insulin BUT is either not producing enough or the insulin it is producing, is not being taken up by cells. Most cases of Diabetes are type 2. It is often seen as a ‘lifestyle’ illness as it is related to obesity, and sedentary lifestyles. Individuals can have diabetes for years before diagnosis.
Current Situation
The patient, a 57-year-old female, diagnosed with Type 2 Diabetes Mellitus (T2DM) in 1996. There is a longstanding history of plantar first MTPJ pain.
Past Medical Hx
Past history of bilateral Achilles tendinopathy; history of paraesthesia in digits 3-5 on the right foot; history of heel burning in the right foot; history of previous bilateral ulceration to the plantar IPJs of the hallux.
Medications
Thyroxine, Metformin, Cilazapril, Vitamins; HbA1c 42mmol/mol (well managed); High BMI 140kg
Goals
To walk pain-free; to increase walking for exercise and weight loss.
Assessment
Key Examination Findings
Pain when palpating the medial and lateral sesamoids of both feet; Achilles tendon midportion thickening present bilaterally. Lateral forefoot squeeze positive for neuritis +/- neuroma; Capillary refill test 3sec bilaterally within normal limits (WNL); DP/PT pulses slightly diminished, bilaterally; Monofilament testing 10/10, bilaterally (WNL) Reflexes WNL bilaterally; True pes cavus foot structure; STJ varum, forefoot in valgum; Forefoot plantarflexed on rearfoot bilaterally; Very plantarflexed first rays; Retracted digits; Limited STJ eversion; Limited weightbearing ankle dorsiflexion; Lateral instability and weak resupination; Thoracic kyphosis, posterior pelvic tilt; General right side hyperloading, statically; Hyperloading 2nd and 5th MT heads, statically; Low weightbearing surface area, statically and dynamically.
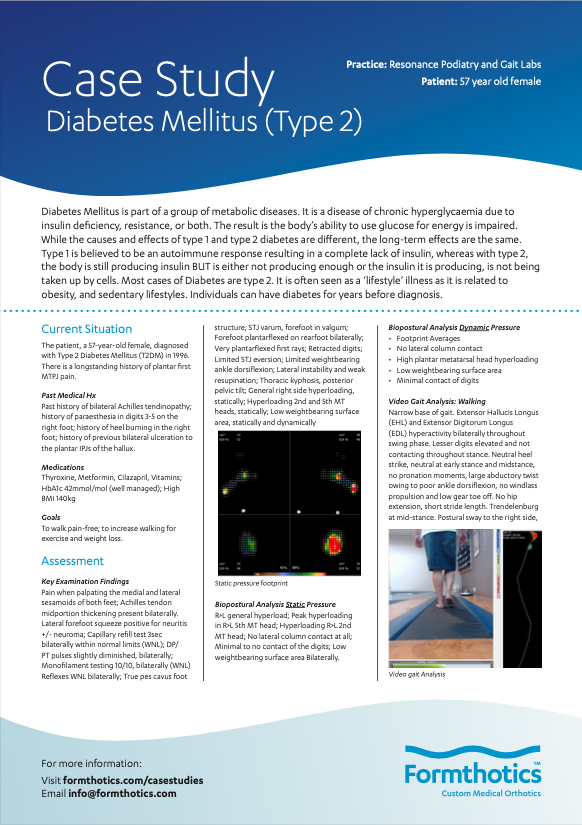
Biopostural Analysis Static Pressure
R>L general hyperload; Peak hyperloading in R>L 5th MT head; Hyperloading R>L 2nd MT head; No lateral column contact at all; Minimal to no contact of the digits; Low weightbearing surface area Bilaterally.
Biopostural Analysis Dynamic Pressure
• Footprint Averages
• No lateral column contact
• High plantar metatarsal head hyperloading • Low weightbearing surface area
• Minimal contact of digits
Video Gait Analysis: Walking
Narrow base of gait. Extensor Hallucis Longus (EHL) and Extensor Digitorum Longus (EDL) hyperactivity bilaterally throughout swing phase. Lesser digits elevated and not contacting throughout stance. Neutral heel strike, neutral at early stance and midstance, no pronation moments, large abductory twist owing to poor ankle dorsiflexion, no windlass propulsion and low gear toe off. No hip extension, short stride length. Trendelenburg at mid-stance. Postural sway to the right side, excessive frontal plane sway. No arm swing.
Diagnosis
This patient has the following risk factors predispose them to future ulceration risk:
T2DM managed via Metformin. History of ulceration to the plantar aspect of the hallux, bilaterally. Pes cavus foot structure, retracted digits. Structural joint limitations and foot deformity. Focal areas of high pressure in the forefoot both statically, and throughout walking gait. High BMI. Lack of exercise. Poor diet. Diminished dorsalis pedis and posterior tibial pulses, bilaterally. Mild par aesthesia onset.
Treatment
- Biomedical Management
- Customised Formthotics
- Footwear changes
- Education regarding daily foot checks
- Annual Diabetic Foot checks
- Referral to Dietician
- Education regarding regular exercise
- HbA1c testing
Management Formthotics Modifications
Dual Density Formthotics- modifications including bilateral lateral posting extending from rearfoot to toes. Bilateral poron metatarsal domes. Bilateral plantar covers with winged cut outs at the first MTPJ, and the fifth MTPJ on the right foot. Additionally, a thin PPT (polypropylene thermoplastic) topcover was added.
The lateral posting modification aims to shift the subtalar joint axis medially in the rearfoot, to decrease supinatory forces, it additionally aims to accommodate the forefoot valgum position and increase weightbearing surface area across the lateral column of the foot, and the lateral forefoot.
The metatarsal dome aims to dorsiflex the metatarsal heads to decrease hyperloading, and evenly distribute pressure across the forefoot. The metatarsal domes aim to decrease pressure on the first metatarsal head, in addition to lateral wedging in the forefoot. Additionally, dorsiflexion of the metatarsal heads aims to reduce contracture of the extensor tendons and reduce retraction of flexible digits.
The plantar cover with the cutouts under the first and fifth MTPJs, directly offload the areas of high pressure, revealed on dynamic and static pressure analysis.
The PPT top cover acts as a cushioning slow release shock absorber to also improve comfort and aid in pressure distribution.
Brooks Dyad walking shoe is a structured neutral shoe option, ideal for stabilising the lateral column to decrease supinatory forces. It has a 12mm heel drop, to increase ground contact in the rearfoot and accommodate the pseudoequinus and increase weightbearing ankle dorsiflexion. Additionally, the full contact outsole of the shoe increases weightbearing surface area and thus shock absorption.
“Maximum peak pressure and time of peak pressure on the foot during gait increases with peripheral neuropathy present.”
“Patients with a history of previous pressure ulceration have higher maximum peak pressures.”
“High plantar pressure variants in conjunction with diabetes duration, smoking, poor glycaemic control, and neuropathy are risk factor for ulceration.”
“Pedobarographic high pressures correlate directly to the site of ulceration, thus high plantar pressures are a useful predictor for foot ulceration in the presence of other comorbidities.”
Outcome
One Month
Resolved plantar first metatarsal (MT)
pain with Formthotics and Footwear. Weightbearing on Formthotics resulted in increased lateral column loading, increased weightbearing surface area. No metatarsal head overload, better weight distribution across the forefoot.
One Year
No ulceration to the plantar aspect of the hallux over 1 year; Increased weight loss- down to 90kgs; Walking – daily; Maintained healthy HbA1c for year; No changes in vascular status, no changes in neuropathic status, vascular and neuro testing all same as previous; Static pressure standing on Modified Formthotics.